Estimation of the arterial stiffness and the biological age
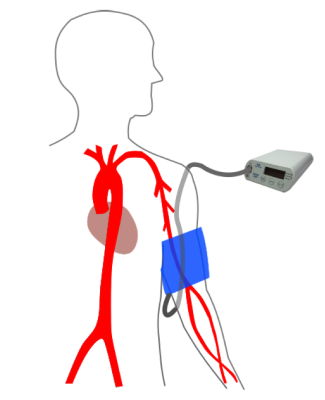
PHYSIO-PORT AS (Arterial Stiffness) uses brand-new algorithms to determine the parameters of arterial stiffness. Blood pressure is measured with our known inflation measurement technic. Immediately afterwards we record the upper arm brachial pulse waves with the help of the blood pressure cuff and the pressure sensor for approximately 15 s.
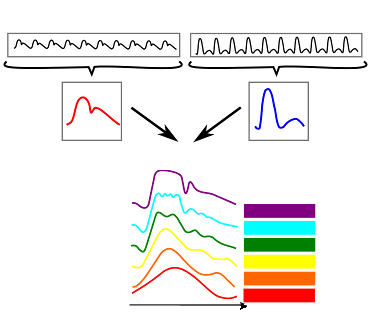
After a special preprocessing of the recorded pulse waves we are able to determine the central pressure waveform with the central blood pressure values. Therefor we use a self-determined transfer function in the frequency domain (Fourier transformation). By that the pulse waves are decomposed in there multiplies of sine and cosine waves. Afterwards the wave parts in the frequency domain are assembled to project the way and the modification of the waves by the vessels between upper arm and the heart. The result is the so called transfer function which is now used to determine the central pressure wave form.
The calculated central pulse wave can be used to determine the parameter of the arterial stiffness. The stiffness of the vessels decreases the Windkessel effect of the elastic vessel walls. The shape of the pulse wave is characteristically modified by the increased reflection of the pressure wave in the vascular system. The physiological aging process results in structural changes of the vascular walls. The vessels will age pathological and will change their structure, if the lifestyle is embossed by risk factors. The combination of the calculated parameters of the arterial stiffness and the risk factors can be used for the primary cardio vascular diagnosis.
Transfer Function
The central pressure waveform is assessed afterwards by pulse wave analysis. We determined the parameters of arterial stiffness which are central blood pressure, augmentation (-index) and pulse wave velocity. The stiffening of the big elastic arteries decreases the arterial Windkessel especially in the aorta. The central arterial wave form changes with increasing blood pressure and lower elasticity in a special assessable way. The parameters of arterial stiffness are surrogates of cardiovascular events and mortality.
Central blood pressure (cSys, cDia)
The central blood pressure is the pressure directly at the heart which means at the beginning of the aorta. This blood pressure has direct impact on left ventricular afterload. In young and healthy persons the big arteries have very elastic vascular walls. The pulse waves from the heart were damped and the reflected wave reaches the heart in diastole. The phenomenon increases the diastolic pressure and therefor ensures a good supply with oxygen-rich blood in the coronary arteries. In case of arterial stiffening the afterload of the left ventricle is too high for a long time. The left ventricular mass decreases which leads to pathophysiological hypertrophy. The oxygen demand increases. With an increased aortic stiffness and high arterial stiffness through the whole arterial tree, reflected pulses waves from the body periphery reach the aorta earlier in systole. The diastolic decreases which lowers the blood supply of the coronary arteries and leads to an even higher central blood pressure than before [1] S.31. The figure on the right visualises the processes.

Augmentation Pressure (AugP) and Augmentationindex (AIx)
The augmentation quantifies the amplification of the central systolic blood pressure by pulse wave reflections (lat. “augmentare” = to amplify) [5] S.133. The augmentation pressure is the amount of pulse pressure, which is added to the forward pulse wave from the heart by pulse wave reflections. The percentage of augmentation pressure on pulse pressure is called augmentationindex (AIx).
Pulse Wave Velocity and Arterial Age (PWV, arterial age ArA)
When the left ventricle contracts it ejects the blood volume and in the same moment a pulse wave comes to the aorta. The velocity of the wave going through the arterial tree is called pulse wave velocity (PWV). The wave induces the so called Windkesseleffekt for damping the strong pulse wave oscillations to generate a continuous blood flow in the smaller arteries. In elastic healthy arteries the pulse wave is reflected in the body periphery and reaches the aorta again in diastole. This increases the diastolic pressure and therefor improves the coronary perfusion. If the elastic function of the arterial wall especially in the aorta gets worse,
the damping function decreases and the pulse wave velocity gets higher. This is why the pulse wave reflections turn back faster and reach the aorta again in early systole, which increase the systolic blood pressure. By that the left ventricle afterload increases. The heart has to work more and in the same moment it is supplied worse because diastolic blood pressure is decreased. The picture visualizes these effects.
The PWV is a direct marker of arterial stiffness and an independent predictor for cardiovascular risk and mortality. Measured PWV values alone or in combination with other tools for risk prediction (e.g. Framingham risk score) are superior in the prediction of cardiovascular events [2] S.8.
The European Heart Journal (P. Boutouyrie et al. 2010 ([4] S. 2344)) defines normal- and reference values for the PWV in different age groups. Data of 16867 persons from 13 study centers were collected. The values were measured mostly with the devices SphygmoCor and Complior. With the PWV measured with PHYSIO-PORT AS in addition with the measured blood pressure from the upper arm it is able to present the (arterial) age of the patient. This value is well understood by patients with high risk potential.
Sources
[1] Mortensen, K. ; Weber, T. ; Baulmann, J.: Arterielle Gefäßsteifigkeit - Biomarker des kardiovaskulären Risikos und ihr Zusammenhang zu kardiovaskulären Erkrankungen. In: Journal für Hypertonie, Austrian Journal of Hypertension 14 (2010), Nr. 2, S. 31–35
[2] Baulmann, J.: Arterielle Gefäßsteifigkeit und Pulswellenanalyse : Positionspapier zu Grundlagen, Methodik, Beeinflussbarkeit und Ergebnisinterpretation. In: DMW,Deutsche Medizinische Wochenschrift 135 (2010), S. 4–14
[3] Palatini, Paolo ; Casiglia ; Gasowski, Jerzy ; Gluszek, Jerzy ; Jankowski ; Narkiewicz;Saladini ; Stolarz-Skrzypek ; Tikhonoff ; Van Bortel ; Wojciechowska ; Kawecka-Jaszcz, K.: Arterial stiffness, central hemodynamics, and cardiovascular risk in hypertension. In: Vascular Health and Risk Management (2011), S. 725
[4] ANR-05-PCOD-004-01: Determinants of pulse wave velocity in healthy people and in the presence of cardiovascular risk factors: 'establishing normal and reference values'. In: European Heart Journal 31 (2010), Nr. 19, S. 2338–2350. URL eurheartj.oxfordjournals.org/content/ehj/31/19/2338.full.pdf – Überprüfungsdatum 2014-11-20
[5] Baulmann, Johannes ; Mortensen, Kai ; Hess, Otto: Wechselwirkung von Arterieller Gefäßsteifigkeit und arterieller Hypertonie – Pathophysiologie, Basisdiagnostik und Messparameter. In: Der Klinikarzt 38 (2009), Nr. 03, S. 132–136